Geneticure Estimates a 250% Increase in Renal Denervation Adoption by Using Genetic Screening to Eliminate Non-responders
Renal denervation has previously demonstrated promise as an interventional procedure that can lower blood pressure (BP) by decreasing signaling of the renal nerves. This can be accomplished using different techniques including radiofrequency/ultrasound ablation or injection of ethanol.
Regardless of denervation method, most studies demonstrate that 1 in 3 patients do not have a meaningful (5mmHg according to the American Heart Association) drop in BP and ~20% of individuals have an increase in BP with renal denervation. Geneticure has developed a cheek-swab genetic screening test to identify those individuals who will not respond to renal denervation. We hypothesize that screening out non-responders will result in a dramatically improved average blood pressure reduction in the remaining renal denervation patient population and increase adoption (250% overall increase in adoption by using genetic screening to increase blood pressure reduction).
A recent study by Medtronic concluded that blood pressure reduction was the most important driver of patient preference over all other attributes like medication burden and treatment (including interventional treatment-related) risks:
- 6.9% of patients would be willing to consider an interventional approach such as RDN with reductions in office blood pressure anticipated at 2.5 mmHg, the minimal acceptable benefit.
- 76.5% of patients would be willing to consider an interventional approach such as RDN with reductions in office blood pressure anticipated at 10 mmHg.
Executive Summary
- Renal denervation has previously demonstrated some promise as an invasive interventional procedure that can lower blood pressure (BP) by decreasing signaling of the renal nerves. For this ablation procedure, a catheter with an ablation tool is introduced through the femoral artery. The renal arteries are then ablated through the walls of the renal artery.
- The initial trials of renal denervation with radiofrequency ablation (Symplicity-HTN-1 and Symplicity-HTN-2) were very promising and demonstrated that patients had a large drop in BP with a denervation procedure when compared to patients who did not have this procedure. However, these studies lacked a control (sham procedure) group.
- Symplicity for HTN-3 included a control group with a sham procedure and the investigators did not find a statistically significant difference between patients who had the procedure and those who did not. Interestingly, some individuals did demonstrate a benefit.
- Regardless of denervation method, most studies demonstrate that 1 in 3 patients do not have a meaningful (5mmHg according to the American Heart Association) drop in BP and ~20% of individuals have an increase in BP with denervation
- Recent data published using a newer denervation device from Medtronic (the Symplicity Spyral™ device) has demonstrated a statistically significant drop in 24-hour systolic blood pressure (SBP) of 3.9mmHG with denervation, when compared to patients who underwent a sham procedure.
- Additional trials from the past two years have demonstrated differences in BP between 0 and 7.4mmHg between renal denervation and a sham procedure.
- A recent meta-analysis of denervation trials using >1300 patients has found an average drop in 24-hour SBP of 3.61mmHg with renal denervation, when compared to sham
- The goal of the Geneticure for Renal Denervation Panel is to identify patients who are likely having a compensatory increase in BP following the procedure and those patients who will likely respond to the denervation procedure. This identification will, ultimately, improve the effectiveness of renal denervation as far as BP reduction in patients with hypertension, increase the number of patients willing to undergo the procedure, and enhance clinical adoption.
- Our hypothesis is that the SNS and cardiac systems are the most important organ systems in individuals who will respond to the denervation procedure, followed closely by the renin-angiotensin-aldosterone system (RAAS, particularly renin, the angiotensin-converting enzyme, and the angiotensin-II receptors) and, finally, the renal (sodium reabsorption) system.
- Patients with functionality in genotypes across all of the organ systems are likely responders to denervation; followed by those with functionality in only the SNS, cardiac, and RAAS systems; then only SNS and cardiac systems, and finally SNS alone.
- In addition, we believe that the patients who are demonstrating a compensatory increase in BP are those with increased sodium reabsorption (due to functional genotypes important in renal sodium handling) following the procedure.
- We genotyped known functional genes within the SNS, cardiac, RAAS, and renal systems and weighted them according to our prediction of how well a patient will respond based on their cumulative genetic score.
Geneticure Hypothesis to Improve Response and Adoption of Renal Denervation
The initial trials of renal denervation with radiofrequency ablation (Symplicity-HTN-1 and Symplicity-HTN-2) were very promising and demonstrated that patients who with a denervation procedure had a large drop in BP when compared to patients who did not have this procedure. However, these studies lacked a control (sham procedure) group. Symplicity for HTN-3 included a control group with a sham procedure and the investigators did not find a statistically significant difference between patients who had the procedure and those who did not. However, some individuals did demonstrate a benefit (figure 1).
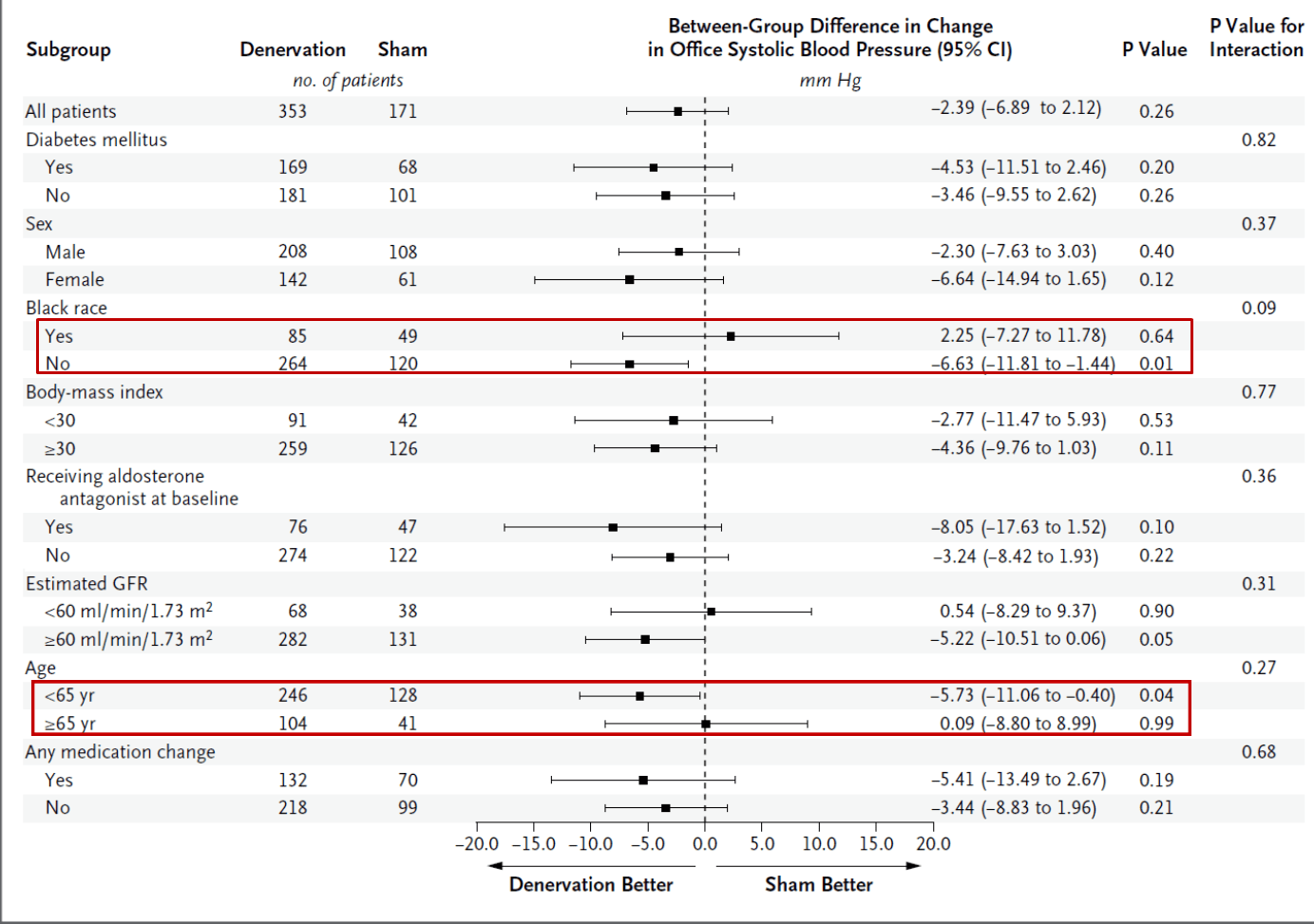
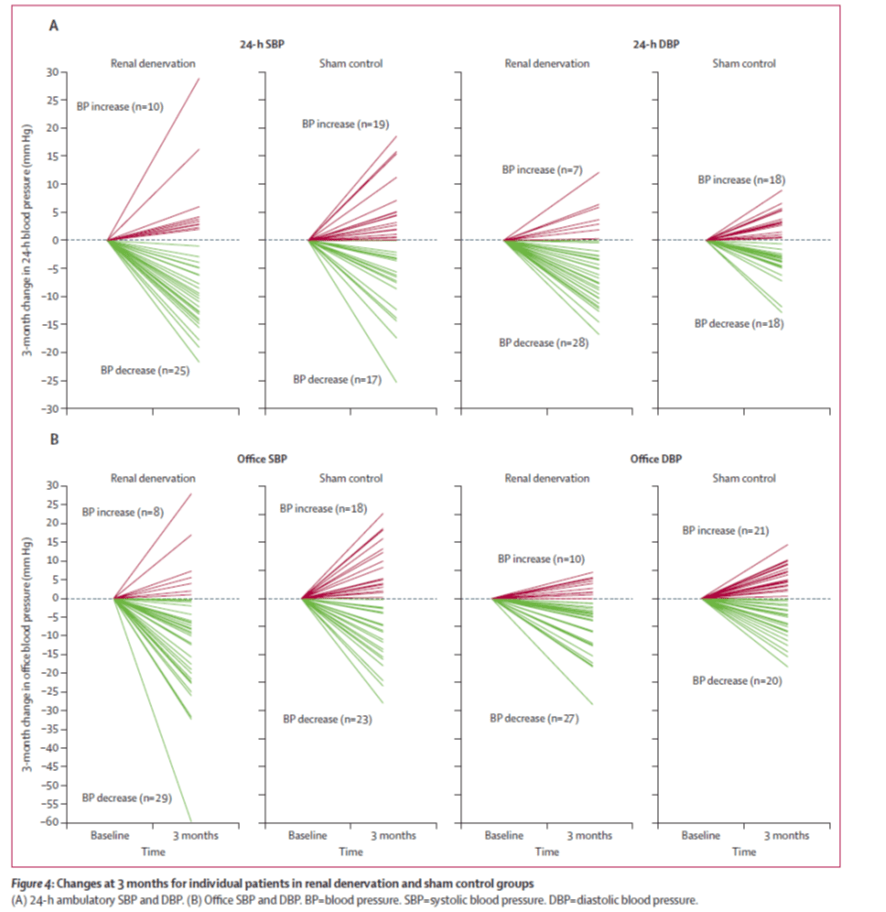
Patients who likely have elevated sympathetic nervous system (SNS) activity (based on age and weight), and patients who have been shown to respond to beta-blockers (based on race) appeared to be a sub-group that demonstrated a drop in blood pressure with the denervation, which initially formed our hypothesis that the genetics of these organ systems can predict responders to renal denervation. Further, regardless of denervation method, most studies demonstrate that 1 in 3 patients do not demonstrate a meaningful (5mmHg according to the American Heart Association) drop in BP and ~20% of individuals have an increase in BP with denervation (red lines denoted in figure 2).
Few Trials are Hitting the American Heart Association Minimum for a Decrease in Blood Pressure
Recent data published using a newer denervation device from Medtronic (the Symplicity Spyral™ device) has demonstrated a statistically significant drop in 24-hour systolic blood pressure (SBP) of 3.9mmHG with denervation, when compared to patients who underwent a sham procedure. Importantly, this trial utilized patients who were not on any medications (SPYRAL OFF-MED trial: Lancet: VOLUME 395, ISSUE 10234, P1444-1451, MAY 02, 2020). Additional trials from the past two years have demonstrated differences in BP between 0 and 7.4mmHg, even when corrected for physiologic variables (i.e. renin and heart rate), and a recent meta-analysis of denervation trials using >1300 patients has found an average drop in 24-hour SBP of 3.61mmHg, when compared to sham (DOI 10.1016/ J.JCIN2021.09.020) (table 1). One recent trial determined that patients in the RDN group required less intensive stepped-up pharmacologic care and fewer hypertension medications when compared to patients in the sham-controlled group (0.9 vs. 1.3 medications in RDN vs sham, respectively); however, this trial also demonstrated a relatively small difference in daytime ambulatory BP between RDN and sham (2.1mmHg, when not corrected for “medication changes”) (DOI 10.1161/ CIRCULATIONAHA.119.040451).
| Company | Technology | Outcome Variable | Treatment Effect Compared to Sham(mmHg) | Effect Corrected for Variable | Year |
| Medtronic | RF Ablation (Off-Med) | 24hr SBP/Office SBP | 3.9mmHg/6.5mmHg | N | 2020 |
| Medtronic | RF (On-Med Proof of Concept) | 24hr SBP/DBP: Office SBP/DBP | 7.4mmHg/4.1mmHg: 6.8mmHg/6.5mmHg | N | 2018 |
| Medtronic | RF (Off-Med) | 24hr SBP/24HR DBP | 5.2mmHg/2.7mmHg | Y (Renin) | 2021 |
| Medtronic | RF (Off-Med) | 24hr SBP | 66.1mmHg | Y (Heart Rate) | 2021 |
| ReCor Medical | Ultrasound (Radiance Trio) | Daytime SBP | ~5mmHg | N | 2021 |
| ReCor Medical | Ultrasound (Require) | 24hr BP | No differences compared to sham | N | 2021 |
| Publication |
| https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30554-7/fulltext |
| https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)30951-6/fulltext |
| https://www.jacc.org/doi/10.1016/j.jacc.2021.04.044 |
| https://www.jacc.org/doi/10.1016/j.jacc.2021.06.044 |
| https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)00788-1/fulltext |
| https://www.nature.com/articles/s41440-021-00754-7 |
Introducing The Geneticure for Renal Denervation Panel
Our hypothesis is that the SNS and cardiac systems are the most important organ systems in individuals who will respond to the denervation procedure, followed closely by the renin-angiotensin-aldosterone system (RAAS, particularly renin, the angiotensin-converting enzyme, and the angiotensin-II receptors) and, finally, the renal (sodium reabsorption) system. Patients with functionality in genotypes across all of the organ systems are likely responders to denervation; followed by those with functionality in only the SNS, cardiac, and RAAS systems; then only SNS and cardiac systems, and finally SNS alone. In addition, we believe that the patients who are demonstrating a compensatory increase in BP are those with increased Na+ reabsorption following the procedure. The organ systems, and the individual genotypes therein, were weighted accordingly for our initial Geneticure for Renal Denervation algorithm. Our hypothesis is underscored with several previous studies in humans and animals that have demonstrated that those with higher SNS activity tend to be responders to renal denervation, that renal denervation acts similar to a beta-blocker in animal models of heart failure, and also alters the expression of the angiotensin-converting enzyme (ACE) and the angiotensin-II receptor.
The goal of the Geneticure for Renal Denervation Panel is to identify patients who are likely having a compensatory increase in BP following the procedure and those patients who will likely respond to the denervation procedure. This identification will, ultimately, improve the effectiveness of renal denervation in this group.
Detailed Background and Hypothesis
Hypertension is one of the most important preventable contributors to disease and death in the world and represents the most common condition seen in the primary care setting[1, 2]. According to the American Heart Association, approximately 78 million adults (1 in 3) living in the United States have hypertension with more than 5 million new diagnoses made each year. Of these individuals, 82% are aware they have it, 75% are currently being treated for it, but only 52% have their blood pressure under control (thus, ~48% do not have adequate blood pressure control). Hypertension is known to lead to myocardial infarction, stroke, renal failure, and death if not detected early and treated appropriately. In fact, in 2009, high blood pressure was listed as a primary or contributing cause of death in ~350,000 of the ~2.4 million U.S. deaths (14% of all deaths). From 1999-2009 the number of deaths attributable to hypertension increased by 44%. In 2009, the direct and indirect economic burden on the United States health care system associated with hypertension was estimated at $51 billion. With the advent of improved diagnostic techniques, increased rates of health care utilization and screening, and the increasing age of the population, a continual upward trend in this expenditure is expected.
Globally, nearly 1 billion individuals have been diagnosed with hypertension with an estimate of an additional 400 million living with undiagnosed hypertension[3]. Hypertension is the leading cause of premature death and the leading cause of cardiovascular disease worldwide. Similar to the upward trend in prevalence as seen in the United States, it is estimated that in 2025 1.56 billion adults will be living with hypertension[4].
Chronic activation of the sympathetic nervous system (SNS) has been identified by preclinical and clinical literature as a common and key factor in disease states such as hypertension, heart failure, and chronic kidney disease[5-7]. The renal sympathetic nerves are a major contributor to the complex pathophysiology of elevated SNS activity and hypertension. Therapeutic renal denervation, the deliberate disruption of the sympathetic nerves connecting the kidneys with the central nervous system, has been shown to be an effective means of modulating elevated SNS activity – both by reducing the sympathetic control of renal function (renin release, sodium excretion and renal blood flow) and by removing the renal afferent sympathetic contribution to central sympathetic elevation[8]. It is important to note that the kidneys maintain appropriate electrolyte and volume homeostasis, despite being denervated, as demonstrated by the human kidney transplant experience[9]. Prior to pharmacological treatment, hypertension was sometimes treated in man with complex invasive procedures, such as surgical nephrectomy and even radical surgical sympathectomy.
The purpose of this the Geneticure for Renal Denervation panel is to assess if a multi-gene panel that contains genes important in SNS function, cardiac function, the renin-angiotensin-aldosterone response, and renal Na+ handling can predict subjects that may have had a differential response to renal denervation using existing data from previous renal denervation trials.
Summary of Previous Research
Integrative Physiology of Hypertension
The development of mechanistic high blood pressure in humans is generally the result of one or more of three physiologic mechanisms: 1) elevated cardiac output (liters of blood ejected from the heart per minute) which increases the amount of blood pressing against the vessels, 2) relatively narrow blood vessels (for a given cardiac output or plasma volume) which results in increased pressure of the blood vessel, or 3) increased sodium (Na+) absorption in the kidney which results in increased blood volume and subsequently increased outward pressure against the vessels. The sympathetic nervous system plays a major role in the development of hypertension. Blood pressure therapy following diagnosis is historically based on an algorithm as suggested by the joint national committee (JNC) of the American Heart Association (AHA) and the American College of Cardiology (ACC)[2]. More recently, the AHA and ACC have updated their guidelines, but adoption to these newer guidelines has been relatively slow. Although national guidelines exist, each hospital system, clinic, and clinician may have their preferred order of pharmacotherapy for hypertension.
Renal Denervation
Renal denervation (or ablation) has been used in animal models and in humans for more than 60 years to reduce blood pressure in patients with resistant hypertension. Renal denervation reduces the signaling (and/or activity) of the sympathetic nerves of the kidney with the three most common methods being radiofrequency, ultrasound, and ethanol ablation. This is a catheter-based procedure through the renal artery and results in a reduction in both efferent and afferent sympathetic signaling [10]. For this ablation procedure, a catheter with an ablation tool is introduced through the femoral artery. The renal arteries are then ablated through the walls of the renal artery with energy applied to the arterial walls. Multiple ablations can be performed with renal ablation typically using several different locations to ensure maximal denervation. This procedure reduces norepinephrine (NE) content within the kidney as well as norepinephrine spillover [10, 11]. The more sites that are ablated, and the closer to the ablation sites are to the renal pelvis, the greater the drop in NE [10]. Early work demonstrated dramatic differences in survival in patients receiving renal denervation-like surgery, vs. those who did not, in a population of resistant hypertensives[12]. Resistant hypertensive patients who underwent thoracolumbar splanchnicectomy had a 54% reduction in mortality over five years, when compared to patients who did not receive the procedure.
More recently, modern surgical devices have been developed to partially ablate the renal nerve in an attempt to control resistant hypertension. The first modern trial on one of these devices, Symplicity HTN-1, was performed on 153 individuals and resulted in substantial reductions in blood pressure for up to three years following the procedure. The average drop in systolic and diastolic blood pressures following renal denervation in Symplicity HTN-1 were 32mmHg and 12mmHg, respectively (compared to no relative change in blood pressure in a control group). Following this initial study, a second trial (Symplicity HTN-2) was performed in which the patients who initially did not receive the renal denervation surgery were allowed to opt-in to the procedure at the 6-month time point for long-term (n=106 total; 52 in the RDN group and 54 in the control group). In both groups (those who had the procedure performed initially and those who had the procedure performed after six months) blood pressure dropped dramatically (31mmHg for systolic blood pressure and 12mmHg for diastolic blood pressure) [13]. These patients also had a reduction in use of renin inhibitors, ACE-inhibitors, and beta-blockers following renal denervation surgery [13]. These changes (drops) in blood pressure persisted to three years post intervention where the average change from baseline was -32.7mmHg and -13.6mmHg for systolic and diastolic blood pressures, respectively.
However, in a sham-controlled trial, Symplicity HTN-3, using a surgical control group that received sham surgery, the investigators demonstrated no difference in blood pressure between those patients who had the sham surgery and those who received renal denervation surgery [2]. This finding has been attributed to number of users (more surgeons in the larger final trial leading some to believe that user error may have played a role), changes in drug regimens, and to the sham control (Hawthorne effect), among other hypotheses.
While Symplicity HTN-3 did demonstrate an effect of RDN (approximately 15mmHg blood pressure reduction, on average), there was no difference when compared to the sham procedure. Further, there was a somewhat larger reduction in blood pressure with Symplicity HTN- 1 and -2 trials, when compared to HTN-3. We hypothesize that the differences among the various patients of Symplicity’s HTN-1 and -2 trials vs. HTN-3 clinical trial are attributable to SNS activity and to genetic variation of genes encoding for the SNS, heart, renin-angiotensin aldosterone system, and for renal Na+ handling of the patients treated.
Renal Denervation and Blood Pressure Regulatory Pathways
Collectively, based on detailed animal studies and more mechanistic studies in humans, renal denervation acts most like a drug that inhibits the SNS, followed by a β-blocker, an ACE-inhibitor/angiotensin-II receptor blocker and least like a diuretic. Renal denervation decreases catecholamine levels within the kidney as well as catecholamine spillover [14, 15] and increases the expression of β1 and β2-adrenergic receptors in the heart (which is a similar physiologic response to β-blockade and demonstrates the importance of these receptors in renal denervation/ablation procedures)(table 2)[14]. In heart failure models, renal denervation improves cardiac function, attenuates left-ventricular hypertrophy, and improves left-ventricular function (similar to the expected response of β-blockade)[16-18]. Renal denervation also decreases the expression (mRNA) of renin, ACE and the angiotensin-II receptors (therefore acting physiologically similar to an ACE-inhibitor and angiotensin-receptor blocker and demonstrating the importance of the renin-angiotensin aldosterone system on renal denervation/ablation). Based on this previous work, we hypothesize that we can use genetics as a means for determining and categorizing very high responders, moderately high responders, moderate responders, minimal responders, and those who are not likely to respond to a renal denervation procedure and have a compensatory increase in blood pressure [19].
| RDx | B-Blockade | Renin Supression | ACE Inhibition | A-II Blockade |
| Improves Cardiac Fx: Decreases LVH and Improved LV fx (EF, end-systolic vs end-diastolic volumes, Ca+ signaling) | x | x | x | x |
| Increases (restores) B1AR and B2AR expression levels | x | |||
| Supress renin, ACE, and ANG-II mRNA in HF and fibrosis models | x (renin) | x | ↑ renin, unless B-blocker used, ↓ ANG-II | |
| Decreases catecholamine levels, SNS, MSNA | x | x |
Response According to Genetic Variants of the Sympathetic Nervous System, Renin-Angiotensin Aldosterone System, the Cardiac System, and the Renal System
Previous research in animals suggests that the functional organ systems having some relation to the renal denervation/ablation procedures are: a) first, the SNS, b) second, the cardiac system, c) third, the renin-angiotensin aldosterone system, and, d) fourth, the renal system. The genes associated with the SNS, cardiac, renin-angiotensin aldosterone system, and renal system may affect the results of renal denervation in a graded, categorized manner. We hypothesize that a subject who will most likely respond to the renal denervation procedure is one who has certain genetic functionalities in the SNS, cardiac system, the renin-angiotensin aldosterone system, AND the renal system. We believe those who will moderately respond are those who have certain functionalities of genes encoding for the SNS, cardiac, AND renin-angiotensin aldosterone system, even in the absence of functionality in the renal system. A subject with functionality in the SNS and cardiac systems but not the renin-angiotensin-aldosterone system will have the next best response. A subject with certain genetic functionalities in the SNS and renin-angiotensin aldosterone system but not the cardiac or renal systems will have a small response to renal denervation/ablation surgery. The purpose of the present pilot study is a first step towards possible categorization of responsiveness to RDN by first assessing if there is an association between multi-gene scoring and changes in BP with denervation.
Sympathetic Nervous System and Cardiac Output
Proteins Important in Cardiac Function
Cardiac output is the amount of blood that is pumped out of the heart per minute and is the product of heart rate (the number of times the heart beats per minute) and stroke volume (SV, the amount of blood ejected from the heart per beat). There are two primary receptors within the heart that influence both rate (chronotropic effect) and contractility (inotropic effect)[20]. The heart is primary comprised of beta-1 adrenergic receptors (β1AR) which are located on 80% of the ventricular wall surface, 70% of the atrial wall surface, and 95% of the sino-atrial (SA) node (which controls heart rate). Although heart rate and cardiac contractility are primarily regulated by the β1AR, the beta-2 adrenergic receptors (β2AR) also play a role, primarily in cardiac contractility[21-23]. Stimulation of either the β1AR or the β2AR influences heart rate and cardiac contractility through increases in intracellular c-AMP and protein kinase A (PKA) which alter Ca+-channel sensitivity and decreases the threshold needed for an action potential. Therefore, cardiac output (and, therefore, blood pressure) is increased through active β1AR or β2ARs (therefore, if a gene that encodes the β1AR or β2AR results in a more functional receptor, cardiac output is higher) following binding from endogenous catecholamines (epinephrine and norepinephrine). Cardiac control is regulated by the autonomic nervous system and elevations in SNS activity lead to an increase in both heart rate and ventricular contractility.
The evidence for the importance of the β1AR and β2AR is demonstrated through the use of selective (i.e. atenolol and metoprolol) and non-selective (i.e. propranolol and carvedilol) beta-blockers (selective meaning they are selective for inhibiting the β1AR and non-selective meaning they inhibit both β1AR and β2AR) which decreased blood pressure through a decrease in heart rate and cardiac contractility. Patients with hypertension often have an augmented sympathetic drive (which is why renal denervation will be of benefit to these patients, according to the hypothesis of the present study) and β-blockade can help to attenuate this elevation in SNS activity. Previous work in animal models has demonstrated that renal denervation reduces the amount of catecholamines circulating in the blood and restores the functionality of the β1 and β2-adrenergic receptors[17, 18, 24]. This is the same effect that a patient with elevated adrenergic drive who is on a β-blocker would experience. Thus, both the β1AR and the β2AR are important in the regulation of cardiac output, and the response to sympathetic nervous system modulation (i.e. renal denervation) with the result of stimulation of these receptors (or more functional receptors due to genetic variation) being elevations in cardiac output (which increases blood pressure unless concurrent vasodilation occurs). Despite the blood pressure reducing effects of both selective and non-selective beta-adrenergic blockade, not all individuals respond similarly to beta-blockade, despite similar clinical and environmental conditions. Black individuals tend to respond poorly to β-blockers, when compared to white individuals[25]. This difference in pharmacodynamic reaction to beta blockade indicates a genetic relation to effectiveness of this class of drugs.
Functional Effects of Genes that Encode Proteins that Influence Sympathetic Nervous System activity and Cardiac Function
There are common and functional alleles of both the alpha-2A and alpha-2C adrenergic receptors that have demonstrated differences in catecholamine and sympathetic response to stimulation. Specifically, the DD variant of the ADRA2C (rs13118711) demonstrates a greater increase in HR, when compared to the II, and ID variants[26]. Further, the D variant demonstrates a greater reduction in norepinephrine levels within 3-months of treatment with Bucindolol, when compared to the I variant [27]. A functional variant of the ADRA2A (rs553668 ) has demonstrated differential BP responses to dexmedetomidine [28] and a functional variant of this gene at a different site (rs2484516) is associated with differential levels of fasting insulin and the insulin response to dexmedetomidine (which can be reflective of SNS activity)[29].
The genes that encode both the β1AR (the gene that encodes this receptor is the ADRB1) and β2AR (the gene that encodes this receptor is the ADRB2) have several functional polymorphisms. These common functional variants alter the protein function, as well as the response to therapy in cell models, animal models, and in human models. Specifically, genetic variation of the ADRB1 at positions 49 (arginine to glycine substitution, rs1801252) and 389 (serine to glycine substitution, rs1801253) influence protein function and response to beta-blockade in humans (table 3)[30]. Individuals with the Arg389 polymorphism of ADRB1 have higher resting blood pressure values, greater left-ventricular mass (which is an adaptation to prolonged elevations in blood pressure), and have a greater response to beta-blockade. Individuals with the Ser49 polymorphism of the have higher resting heart rate and blood pressure values and are, therefore, more responsive to a beta-blocker.
Within the gene that encodes the ADRB2, amino acids 16 and 27 have common functional variants with the glycine polymorphism at position 16 being more prevalent in hypertensives and people with this variant demonstrating higher resting stroke volume and cardiac output[14, 23, 31-33]. In addition, the arginine variant at position 16 of the ADRB2 has higher levels of mortality following beta-blockade after acute coronary syndrome. The glutamine variant at amino acid 27 of the ADRB2 (Glu27) is more prevalent in patients with hypertension.
The distribution of the alpha adrenergic and β1 and β2-adrenergic receptor variants differs significantly among different racial groups, particularly between white and black individuals.
| Organ System | Gene/Variant | rs# | Importance in Renal Denervation |
| Sympathetic Tone | ADRA2A | 2484516 | High |
| ADRA2A | 553668 | Very High | |
| ADRA2C Del | 13118711 | Extremely High | |
| Heart (Cardiac Output) | ADRB2_16 | 1042713 | High |
| ADRB2_27 | 1042714 | High | |
| ADRB1_49 | 1801252 | Extremely High | |
| ADRB1_389 | 1801253 | Extremely High |
Renin-Angiotensin Aldosterone System and Vascular Function
Dilation of blood vessels results in decreases in blood pressure, whereas constriction of blood vessels results in increases in blood pressure. Blood vessel diameter is controlled through local neural signaling (parasympathetic control) as well as circulating hormones (sympathetic control) and other circulating proteins. Accordingly, blood pressure increases with elevations in sympathetic drive, which is likely attenuated with renal denervation/ablation. The angiotensin receptors are stimulated by angiotensin II which is converted from angiotensin I through the angiotensin converting enzyme (ACE). Angiotensin-II is a potent vasoconstrictor and actively acts to inhibit bradykinin which is a potent vasodilator, having a dual role in vasoconstriction. Therefore, a common target of blood pressure therapy through promotion of vasodilation is through the inhibition of the activity of ACE (i.e. ACE inhibitors), which reduces the bioavailability of angiotensin-II. Similarly, angiotensin-II receptor antagonists work through the competitive inhibition of the angiotensin-II receptors which decreases the number of receptors that are available to bind to angiotensin II.
Functional Effects of Genes that Encode Proteins that Influence Vascular Function
Several common and functional polymorphisms of the genes that encode for ACE and A-II receptors have been described. These genotypes alter protein function, as well as the response to drug therapies in cell models, animal models, and human models (table 4). Within the gene that encodes ACE, there is one known common and functional polymorphism (rs1799752), an insertion or deletion polymorphism of a 287 base pair fragment [34]. The deletion polymorphism of ACE results in higher plasma levels of ACE and a greater drop in ejection fraction in patients following MI [35, 36]. In addition, patients with the deletion polymorphism have left-ventricular hypertrophy at higher rates when compared to patients with the insertion polymorphism (left-ventricular hypertrophy results secondary to prolonged exposure to high blood pressure).
Therefore, we hypothesize that the deletion polymorphism of ACE would provide a response to renal denervation.
At least three functional variants of angiotensin have been found to be common in humans (rs5051, rs699, and rs7079)[37, 38]. Functional polymorphisms of angiotensin results in higher angiotensin levels and higher resting blood pressure values. Therefore, according to the hypothesis, patients with these genetic variants will benefit more from renal denervation due to a greater effect on the blunting of ACE and the angiotensin-II receptor.
A common functional polymorphism of an angiotensin receptor (type-I) has been described (rs5186)[39, 40] and influences resting blood pressure values and demonstrates which patients will benefit more from renal denervation due to attenuation of angiotensin-II expression. Specifically, patients with the C variant of the angiotensin receptor type I have higher resting blood pressure values, more detrimental cardiovascular events, and have a greater chance of developing high blood pressure during pregnancy, when compared to the A variant. Collectively, the C variant will be more responsive to renal denervation.
In addition to angiotensin, angiotensin II receptors and ACE, renin has been shown to be a potent vasoconstrictor that can result in high blood pressure. Renin converts angiotensinogen to angiotensin I which results in vasoconstriction due to the down-stream effects (angiotensin-I conversion to angiotensin II through ACE). There is one functional and common polymorphism of renin that demonstrates an altered blood pressure response to vasodilator therapy, a cytosine to threonine substitution at nucleotide 5312 (rs12750834)[15]. Within this polymorphism of renin, the thymine substitution and the heterozygous condition demonstrate higher renin levels as well as a greater reduction in blood pressure in response to valsartan (which is an angiotensin II receptor blocker). Given that renal denervation surgery results in attenuation of renin release and ACE activity, along with down-regulation of the angiotensin-II receptor, according to the hypothesis of the present study, this same variant (thymine) of renin will be one that responds better to renal denervation therapy.
| Organ System | Gene/Variant | rs# | Importance in Renal Denervation |
| Vessels (vascular dilation/constriction) | Renin | 12750834 | Extremely High |
| Angiotensin | 5051 | High | |
| Angiotensis | 699 | High | |
| Angiotensin | 7079 | High | |
| ACE | 1799752 | Extremely High | |
| AII Receptor | 5186 | Extremely High |
Sodium (Na+) Reabsorption in the Kidney
Proteins Important in Renal Na+ Reabsorption
Many consider the kidneys to be the center of long-term blood pressure regulation. Alterations in Na+ reabsorption in the kidneys results in alterations in fluid retention, which leads to increases or decreases in blood plasma volume and changes the pressure against the vessels. There are several proteins that are important in renal Na+ handling and the response to diuretic therapy including the epithelial Na+ channels (SCNN1A, rs2228576), alpha-adducin (rs4961), the Na+Cl- co-transporter (rs159927), and lysine deficient protein kinase -1 (WNK, rs1159744, rs2106714, and rs2277869). The epithelial sodium (Na+) channel is responsible for Na+ reabsorption on the apical portion of epithelial cells in the kidneys. The epithelial Na+ channel is made up of three different subunits; the alpha, beta, and gamma. The alpha subunit of the epithelial Na+ channel is highly functional and removal of this subunit abolishes channel activity in cell and animal models. The gamma subunit is also extremely important in channel function and functional genetic variants of this channel result in pseudohypoaldosteronism type-I and Liddle’s syndrome, two severe genetic diseases resulting in salt wasting and high salt conservation (salt sensitivity), respectively. Adducin is made up of an alpha, beta, and gamma subunit. The alpha subunit of adducin increases sodium (Na+) reabsorption in the kidneys through activity of Na+K+ ATPase (which moves Na+ and potassium into out of cells). The sodium (Na+) chloride (Cl-) co-transporter is important in regulating Na+ and Cl- movement between the kidney and the rest of the body. Active Na+-Cl- transport results in Na+ reabsorption and, therefore, results in higher blood pressure. The WNK1 protein is a key regulator of long-term Na+ and chloride Cl- reabsorption in the kidneys. WNK1 regulates the activity of Na+-Cl- co-transporters. If a patient has a more active WNK1 genotype, they have greater Na+ and Cl- reabsorption in the kidneys which increases blood volume and, therefore, the pressure on the vessels.
Increases in the activity of the proteins important in renal Na+ and Cl- regulation result in increases in Na+ retention and elevations in blood pressure. It is also, therefore, likely that these genetic variations also enable a greater response renal denervation, when considered in the presence of functional variants of the renin-angiotensin aldosterone system and the cardiac system.
Functional Effects of Genes that Encode Proteins that Influence Renal Na+ Reabsorption
A functional and common polymorphism of the gene that encodes the epithelial Na+ channel (SCNN1A) has been identified (alanine to threonine substitution at position 663)(table 5). Patients with the threonine substitution of SCNN1A have more functional Na+ channels (higher activity and higher voltage currents across the cells) and are more susceptible to hypertension[41-43]. Common and functional genetic variation of alpha adducin has also been identified (glycine to tryptophan substitution at amino acid 460). Within alpha adducin, individuals with the tryptophan variant are more likely to be salt sensitive, have higher rates of hypertension and have demonstrated a greater response to a diuretic[44, 45]. Genetic variation of the sodium (Na+) chloride (Cl-) co-transporter (SLC12A3) also demonstrates functional consequences. Within the SLC12A3, patients with the alanine variant have a better response to loop diuretics and demonstrate more excretion of Cl- and K+ in response to diuretic therapy. Patients with the cytosine variant of WNK at genes rs1159744 and rs2107614 have greater blood pressure reductions in response to diuretic therapy when compared to patients with the glycine or threonine variants at these two sites, respectively[46].
It is, therefore, likely that hypertensive patients with a functional polymorphism of the SCNN1A (threonine 663) variant), ADD1 (tryptophan 460 variant), SLC12A3 (alanine 264 variant), and WNK (cytosine for rs1159744, rs227869, and rs2107614) will be most responsive to renal denervation surgery, particularly when all are functional and when the renal system is considered along with the renin-angiotensin aldosterone and cardiac systems.
| Organ System | Gene/Variant | rs# | Importance in Renal Denervation |
| Kidney (Na+ regularion: plasma volume) | Alpha Adducin | 491 | Average |
| SCNN1a | 2228576 | Average | |
| SLC12A3 (2) | 1529927 | Average | |
| WNK1(a) | 1159744 | High | |
| WNK1(b) | 2107614 | High | |
| WNK1(c) | 2277869 | Average |
Association Between a Multi-Gene Panel and Renal Denervation Effectiveness in Patients With Hypertension
ClinicalTrials.gov Identifier: NCT04060641
Study Purpose and Hypothesis
Geneticure, Inc. is currently assessing the influence of our multi-gene panel on the blood pressure response to renal denervation. The purpose of this study is to assess the relationship between the ranked score of the Geneticure multigene panel for renal denervation success and the blood pressure response to renal denervation. This study will be performed as a retrospective study on patients who have participated in a renal denervation trial, have reached the primary efficacy endpoint, received renal denervation and agree to participate. The study will involve collection of DNA via a buccal swab and a clinical chart review of the patient’s hypertension and medication history. From the buccal swab we will assess 20 SNPs: (2) SNPs in ADRA2A, (1) SNP in ADRA2C, (2) SNPs in ADRB1, (2) SNPS in ADRB2, (1) in SCNN1A, (1) in ADD1, (2) in SLC12A3, (3) in WNK1, (1) in ACE, (3) in AGT, and (1) each in AGTR1, and REN with known functionality in the SNS, heart, vasculature, and kidney.
The present study will assess if subjects who have a high genetic score, based on the hypothesized importance of the organ systems involved, will have differential responsiveness to RDN in a descending order. The genetic scoring is collectively ranked in a specific order, in that:
- Subjects with a “high level of general functionality” (functionality in the sympathetic nervous system (SNS), cardiac, vascular (renin-angiotensin-aldosterone system (RAAS)), and renal system genotypes will be most responsive to RDN.
- Subjects with high number of functional genotypes of SNS, cardiac, and RAAS will be the next most responsive group.
- Subjects with functionality in genotypes of SNS and cardiac systems will demonstrate the next most responsive group.
- Subjects with functionality in the SNS genotypes will demonstrate some degree of responsiveness.
- Subjects with functionality in the renal system, but not SNS, cardiac, nor RAAS, will be the least responsive to this therapy and are likely the group demonstrating a compensatory increase in BP following renal denervation.
References
- Kearney, P.M., M. Whelton, K. Reynolds, et al., Global burden of hypertension: analysis of worldwide data. Lancet, 2005. 365(9455): p. 217-23.
- James, P.A., S. Oparil, B.L. Carter, et al., 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA, 2014. 311(5): p. 507-20.
- Sakhuja, A., S.C. Textor and S.J. Taler, Uncontrolled hypertension by the 2014 evidence-based guideline: results from NHANES 2011-2012. J Hypertens, 2015. 33(3): p. 644-51; discussion 652.
- Qamar, A. and E. Braunwald, Treatment of Hypertension: Addressing a Global Health Problem. JAMA, 2018. 320(17): p. 1751-1752.
- Charkoudian, N. and J.A. Rabbitts, Sympathetic neural mechanisms in human cardiovascular health and disease. Mayo Clin Proc, 2009. 84(9): p. 822-30.
- Joles, J.A. and H.A. Koomans, Causes and consequences of increased sympathetic activity in renal disease. Hypertension, 2004. 43(4): p. 699-706.
- Mancia, G., G. Grassi, C. Giannattasio, et al., Sympathetic activation in the pathogenesis of hypertension and progression of organ damage. Hypertension, 1999. 34(4 Pt 2): p. 724-8.
- Krum, H., M. Schlaich, R. Whitbourn, et al., Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet, 2009. 373(9671): p. 1275-81.
- Coruzzi, P., L. Musiari, G.L. Mossini, et al., The renin-aldosterone system and renal function in kidney transplantation. Clin Nephrol, 1994. 41(4): p. 225-9.
- Schlaich, M.P., Renal Sympathetic Denervation: A Viable Option for Treating Resistant Hypertension. Am J Hypertens, 2017. 30(9): p. 847-856.
- Li, Z.Z., H. Jiang, D. Chen, et al., Renal sympathetic denervation improves cardiac dysfunction in rats with chronic pressure overload. Physiol Res, 2015. 64(5): p. 653-62.
- Smithwick, R.H. and J.E. Thompson, Splanchnicectomy for essential hypertension; results in 1,266 cases. J Am Med Assoc, 1953. 152(16): p. 1501-4.
- Symplicity, H.T.N.I., M.D. Esler, H. Krum, et al., Renal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 Trial): a randomised controlled trial. Lancet, 2010. 376(9756): p. 1903-9.
- Snyder, E.M., S.T. Turner, M.J. Joyner, et al., The Arg16Gly polymorphism of the β2-adrenergic receptor and the natriuretic response to rapid saline infusion in humans. J Physiol, 2006. 574(Pt 3): p. 947-54.
- Vangjeli, C., N. Clarke, U. Quinn, et al., Confirmation that the renin gene distal enhancer polymorphism REN-5312C/T is associated with increased blood pressure. Circ Cardiovasc Genet, 2010. 3(1): p. 53-9.
- Tsioufis, C., K. Dimitriadis, C. Thomopoulos, et al., Renal and cardiac effects of renal sympathetic denervation and carotid baroreceptor stimulation. Curr Vasc Pharmacol, 2014. 12(1): p. 55-62.
- Pinkham, M.I., M.T. Loftus, S. Amirapu, et al., Renal denervation in male rats with heart failure improves ventricular sympathetic nerve innervation and function. Am J Physiol Regul Integr Comp Physiol, 2017. 312(3): p. R368-R379.
- Watanabe, H., Y. Iwanaga, Y. Miyaji_, et al., Renal denervation mitigates cardiac remodeling and renal damage in Dahl rats: a comparison with beta-receptor blockade._ Hypertens Res, 2016. 39(4): p. 217-26.
- Gupta, A.K., Racial differences in response to antihypertensive therapy: does one size fits all? Int J Prev Med, 2010. 1(4): p. 217-9.
- Brodde, O.E., The functional importance of beta 1 and beta 2 adrenoceptors in the human heart. Am J Cardiol, 1988. 62(5): p. 24C-29C.
- Bristow, M.R., R.E. Hershberger, J.D. Port, et al., Beta 1- and beta 2-adrenergic receptor-mediated adenylate cyclase stimulation in nonfailing and failing human ventricular myocardium. Mol Pharmacol, 1989. 35(3): p. 295-303.
- Busjahn, A., G.-H. Li, H.-D. Faulhaber, et al., β-2 Adrenergic Receptor Gene Variations, Blood Pressure, and Heart Size in Normal Twins. Hypertension, 2000. 35(2): p. 555-560.
- Snyder, E.M., K.C. Beck, N.M. Dietz, et al., Arg16Gly polymorphism of the β2-adrenergic receptor is associated with differences in cardiovascular function at rest and during exercise in humans. J Physiol, 2006. 571(Pt 1): p. 121-30.
- Dhakal, P., K. Liu, H. Kozman, et al., Renal Denervation in Heart Failure: A New Therapeutic Paradigm. Clin Med Insights Cardiol, 2015. 9(Suppl 1): p. 101-4.
- Shekelle, P.G., M.W. Rich, S.C. Morton, et al., Efficacy of angiotensin-converting enzyme inhibitors and beta-blockers in the management of left ventricular systolic dysfunction according to race, gender, and diabetic status: a meta-analysis of major clinical trials. J Am Coll Cardiol, 2003. 41(9): p. 1529-38.
- Kurnik, D., E.A. Friedman, M. Muszkat, et al., Genetic variants in the alpha2C-adrenoceptor and G-protein contribute to ethnic differences in cardiovascular stress responses. Pharmacogenet Genomics, 2008. 18(9): p. 743-50.
- Bristow, M.R., G.A. Murphy, H. Krause-Steinrauf, et al., An alpha2C-adrenergic receptor polymorphism alters the norepinephrine-lowering effects and therapeutic response of the beta-blocker bucindolol in chronic heart failure. Circ Heart Fail, 2010. 3(1): p. 21-8.
- Kurnik, D., M. Muszkat, C. Li, et al., Genetic variations in the alpha(2A)-adrenoreceptor are associated with blood pressure response to the agonist dexmedetomidine. Circ Cardiovasc Genet, 2011. 4(2): p. 179-87.
- Ghimire, L.V., M. Muszkat, G.G. Sofowora, et al., Variation in the alpha(2A) adrenoceptor gene and the effect of dexmedetomidine on plasma insulin and glucose. Pharmacogenet Genomics, 2013. 23(9): p. 479-86.
- Johnson, J.A. and S.T. Turner, Hypertension pharmacogenomics: current status and future directions. Curr Opin Mol Ther, 2005. 7(3): p. 218-25.
- Snyder, E.M., M.L. Hulsebus, S.T. Turner, et al., Genotype Related Differences in beta2 Adrenergic Receptor Density and Cardiac Function. Med Sci Sports Exerc, 2006. 38(5): p. 882-6.
- Snyder, E.M., B.D. Johnson and M.J. Joyner, Genetics of beta2-adrenergic receptors and the cardiopulmonary response to exercise. Exerc Sport Sci Rev, 2008. 36(2): p. 98-105.
- Snyder, E.M., M.J. Joyner, S.T. Turner, et al., Blood pressure variation in healthy humans: a possible interaction with beta-2 adrenergic receptor genotype and renal epithelial sodium channels. Med Hypotheses, 2005. 65(2): p. 296-9.
- Ulgen, M.S., O. Ozturk, S. Alan, et al., The relationship between angiotensin-converting enzyme (insertion/deletion) gene polymorphism and left ventricular remodeling in acute myocardial infarction. Coron Artery Dis, 2007. 18(3): p. 153-7.
- McNamara, D.M., R. Holubkov, L. Postava, et al., Pharmacogenetic interactions between angiotensin-converting enzyme inhibitor therapy and the angiotensin-converting enzyme deletion polymorphism in patients with congestive heart failure. J Am Coll Cardiol, 2004. 44(10): p. 2019-26.
- Pilati, M., M. Cicoira, L. Zanolla, et al., The role of angiotensin-converting enzyme polymorphism in congestive heart failure. Congest Heart Fail, 2004. 10(2): p. 87-93; quiz 94-5.
- Pilbrow, A.P., B.R. Palmer, C.M. Frampton, et al., Angiotensinogen M235T and T174M gene polymorphisms in combination doubles the risk of mortality in heart failure. Hypertension, 2007. 49(2): p. 322-7.
- Tang, W., R.B. Devereux, D.C. Rao, et al., Associations between angiotensinogen gene variants and left ventricular mass and function in the HyperGEN study. Am Heart J, 2002. 143(5): p. 854-60.
- Miller, J.A., K. Thai and J.W. Scholey, Angiotensin II type 1 receptor gene polymorphism predicts response to losartan and angiotensin II. Kidney Int, 1999. 56(6): p. 2173-80.
- Baudin, B., Angiotensin II receptor polymorphisms in hypertension. Pharmacogenomic considerations. Pharmacogenomics, 2002. 3(1): p. 65-73.
- Meisler, M.H., L.L. Barrow, C.M. Canessa, et al., SCNN1, an epithelial cell sodium channel gene in the conserved linkage group on mouse chromosome 6 and human chromosome 12. Genomics, 1994. 24(1): p. 185-6.
- Jin, H.S., K.W. Hong, J.E. Lim, et al., Genetic variations in the sodium balance-regulating genes ENaC, NEDD4L, NDFIP2 and USP2 influence blood pressure and hypertension. Kidney Blood Press Res, 2010. 33(1): p. 15-23.
- Pratt, J.H., Central role for ENaC in development of hypertension. J Am Soc Nephrol, 2005. 16(11): p. 3154-9.
- Zhang, L.N., L.D. Ji, L.J. Fei, et al., Association between polymorphisms of alpha-adducin gene and essential hypertension in Chinese population. Biomed Res Int, 2013. 2013: p. 451094.
- Psaty, B.M., N.L. Smith, S.R. Heckbert, et al., Diuretic therapy, the alpha-adducin gene variant, and the risk of myocardial infarction or stroke in persons with treated hypertension. JAMA, 2002. 287(13): p. 1680-9.
- Turner, S.T., G.L. Schwartz, A.B. Chapman, et al., WNK1 kinase polymorphism and blood pressure response to a thiazide diuretic. Hypertension, 2005. 46(4): p. 758-65.